
Flying by the Seat of Your Pants in BPPV: Why You Always Treat Away from the Strongest Nystagmus in Horizontal Canal - BPPV (GEO or APO)
By Brian Werner, PT, MPT - National Director of Education & Training - FYZICAL, LLC
As a physical therapist specializing in vestibular and balance disorders for over a quarter of a century, I have seen countless patients with Benign Paroxysmal Positional Vertigo (BPPV). When a patient presents with horizontal canal BPPV, you observe one of two types of nystagmus: geotropic or apogeotropic. Geotropic nystagmus beats toward the Earth, while apogeotropic nystagmus beats away from the Earth. Understanding the difference and knowing which side to treat can feel like you are 'flying by the seat of your pants,' but a core principle for horizontal canal BPPV is simple: you always treat away from the strongest nystagmus. The physics of where the otoconia (debris) are located within the horizontal semicircular canal dictate this rule.
It is a fascinating aspect of our profession, one that even seasoned clinicians like myself might unconsciously apply without fully appreciating the elegant simplicity it offers in treatment. Yes, the diagnostic process involves careful observation and differentiation, but when it comes to the actual treatment, a single, powerful rule emerges.
Understanding the Supine Head Roll Test
You use the Supine Head Roll Test to differentiate between geotropic and apogeotropic BPPV and determine the affected ear. The intensity of the nystagmus you observe tells you everything you need to know. The following table provides a quick guide to understanding which side is affected.
The table reinforces a simple, unifying principle for treatment: the affected ear is always the one opposite the side with the strongest nystagmus.
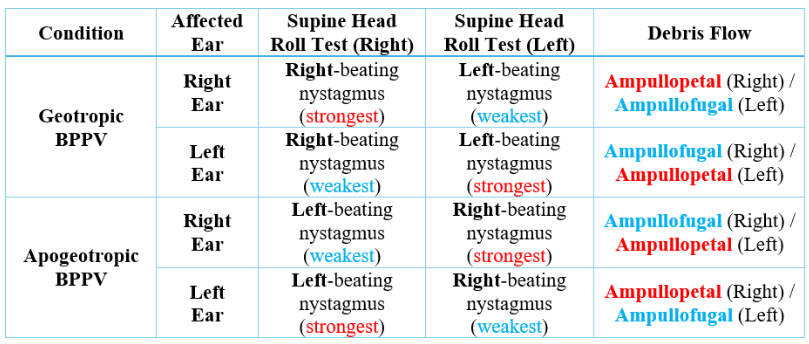
This chart is an overview of HSC-BPPV and the strong side of the nystagmus.
Geotropic HSC-BPPV: The Logic
In Geotropic HSC-BPPV, the otoconia are located in the non-ampullary arm of the horizontal canal, which is the longer segment of the canal furthest from the ampulla. When you perform a Supine Head Roll Test to the affected side, gravity pulls the otoconia ampullopetally (toward the ampulla). This movement excites the canal, causing a strong nystagmus.
GIF 1: Starting with a Supine Head Roll Test (SHRT) to the LEFT, you see the movement of debris. The blue arrow (GEO) represents an inhibitory response, while the red arrow (GEO) represents an excitatory response. We know the affected ear is the RIGHT side - we treat AWAY FROM the strong side. This would be the LEFT side.
You must move the debris out of the canal and back into the utricle. To achieve this, you must roll the patient in a way that continues the momentum of the debris's movement. Therefore, for geotropic BPPV, you treat the patient by moving them away from the side that produced the strongest nystagmus (which is also the affected side) and toward the unaffected side. You commonly achieve this with a Gufoni, Lempert, or the Quick maneuver.
GIF 2: Starting with a Supine Head Roll Test (SHRT) to the LEFT, you see the movement of debris. The red arrow (GEO) represents an excitatory response, while the blue arrow (GEO) represents an inhibitory response in SHRT to the RIGHT. We know the affected ear is the LEFT side - we treat AWAY FROM the strong side. This would be the RIGHT side.
Apogeotropic HSC-BPPV: The Same Principle, Different Manifestation
In Apogeotropic HSC-BPPV, the otoconia are primarily in the ampullary arm of the horizontal canal, which is the segment closer to the ampulla.
Please note: it is well understood that debris for apogeotropic HSC-BPPV can be in many places, including the short arm and periampullary regions on both sides of the cupula. In this example, we are treating the ampullary arm (anterior arm HSC-BPPV).When you perform a Supine Head Roll Test to the affected side, gravity pulls the otoconia ampullofugally (away from the ampulla). This movement inhibits the canal, resulting in less intense nystagmus. However, when you roll the patient's head to the opposite, unaffected side, gravity pulls the otoconia ampullopetally (toward the ampulla), creating an excitatory movement and a stronger nystagmus.
GIF 3: Starting with a Supine Head Roll Test (SHRT) to the LEFT, you see the movement of debris. The red arrow represents an excitatory response (APO), while the blue arrow (APO) represents an inhibitory response in the SHRT to the RIGHT. We know the affected ear is the RIGHT side - we treat AWAY FROM the strong side. This would be the RIGHT side.
We know the affected ear is on the right side - we treat AWAY FROM the strong ear side. We treat the right side.
The side with the strongest nystagmus is the unaffected side. To treat the affected ear, which exhibits weaker nystagmus, you still roll the patient away from the stronger nystagmus. This means moving them towards the affected ear in this specific apogeotropic scenario. This treatment is a Zuma Maneuver, Inverted Gufoni (Appiani/Vannucchi-Asprella - modified), or Casani maneuver, but the direction of the roll is what makes the crucial difference.

GIF 4: Starting with a Supine Head Roll Test (SHRT) to the LEFT, you see the movement of debris. The blue arrow (APO) represents an inhibitory response, while the red arrow (APO) represents an excitatory response when doing SHRT to the RIGHT. We know the affected ear is the LEFT side - we treat AWAY FROM the strong side. This would be the LEFT side.
We know the affected ear is on the left side - we treat AWAY FROM the strong ear side. We treat the left side.
The Bottom Line: Horizontal Canal BPPV Simplified
Whether the presentation is geotropic or apogeotropic, the treatment principle for horizontal canal BPPV remains elegantly simple. You are always treating the affected ear by rolling the patient away from the side that produced the most robust nystagmus. This ensures you leverage gravity to move the otoconia out of the semicircular canal and back into the utricle, where they belong, resolving the patient's debilitating vertigo.
Important Note: This principle is specific to the horizontal canal and should not be applied to the vertical canals (posterior and anterior BPPV), as their unique anatomy and treatment algorithms differ.